

References:
- DARZALEX® [Prescribing Information]. Horsham, PA: Janssen Biotech, Inc.
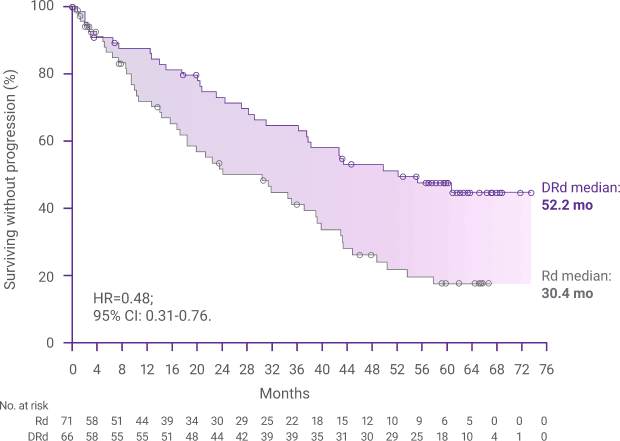
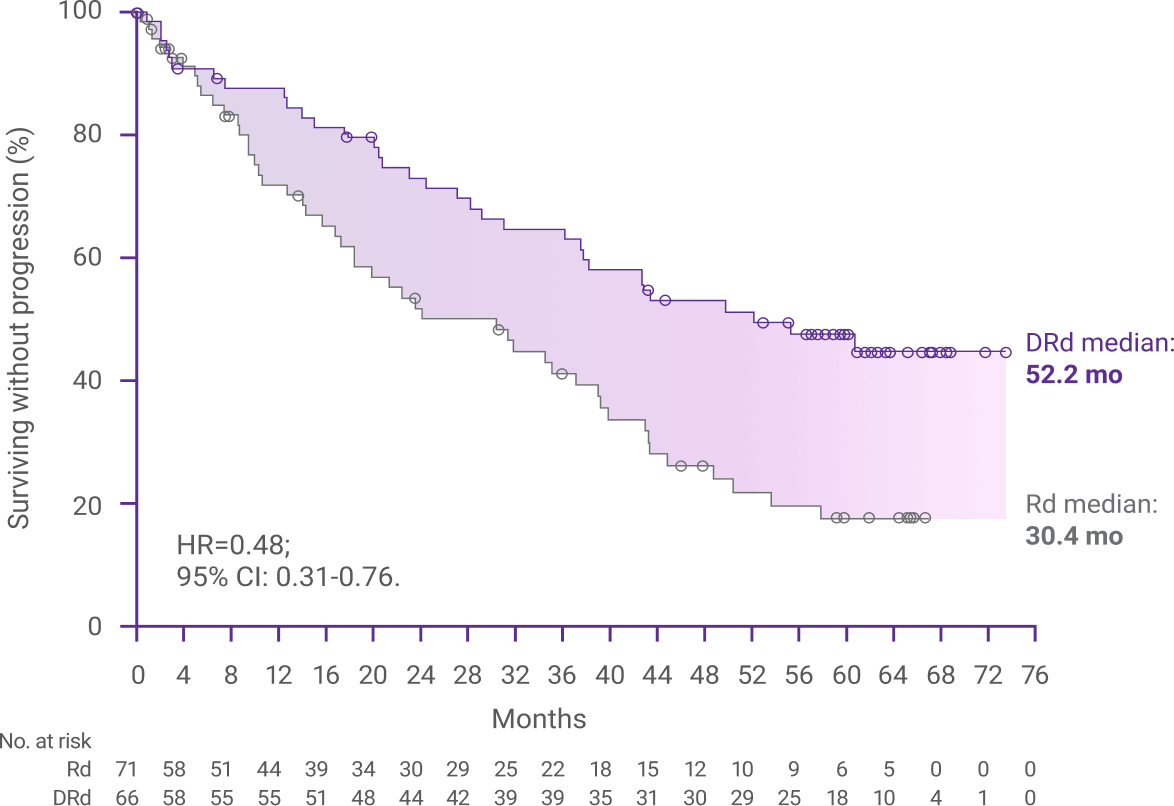
- Facon T, Kumar S, Plesner T, et al; the MAIA Trial Investigators. Daratumumab plus lenalidomide and dexamethasone for untreated myeloma. N Engl J Med. 2019;380(22):2104-2115.
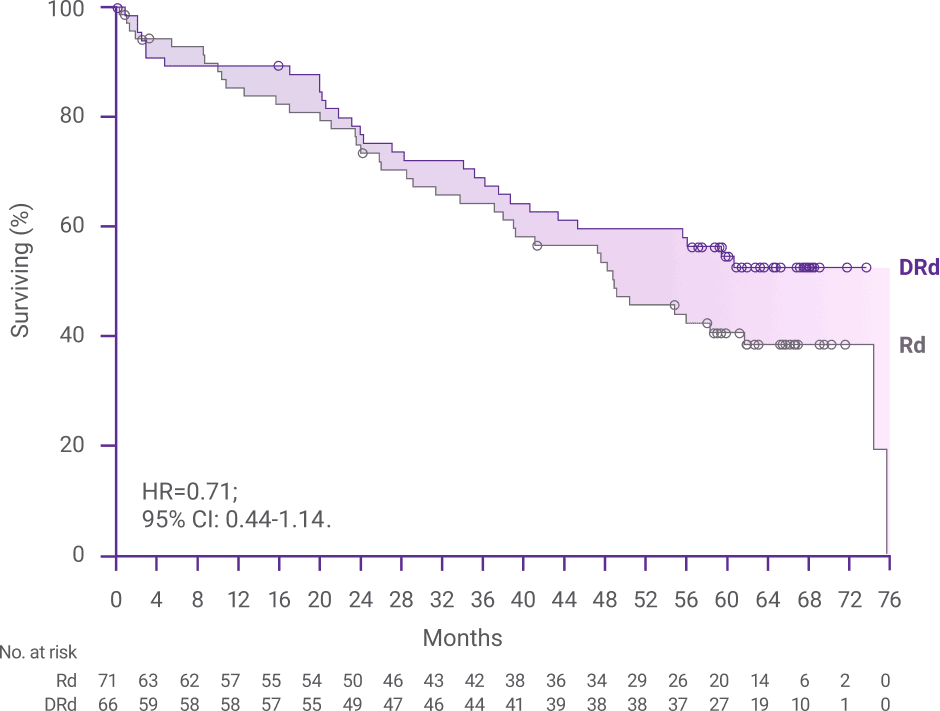
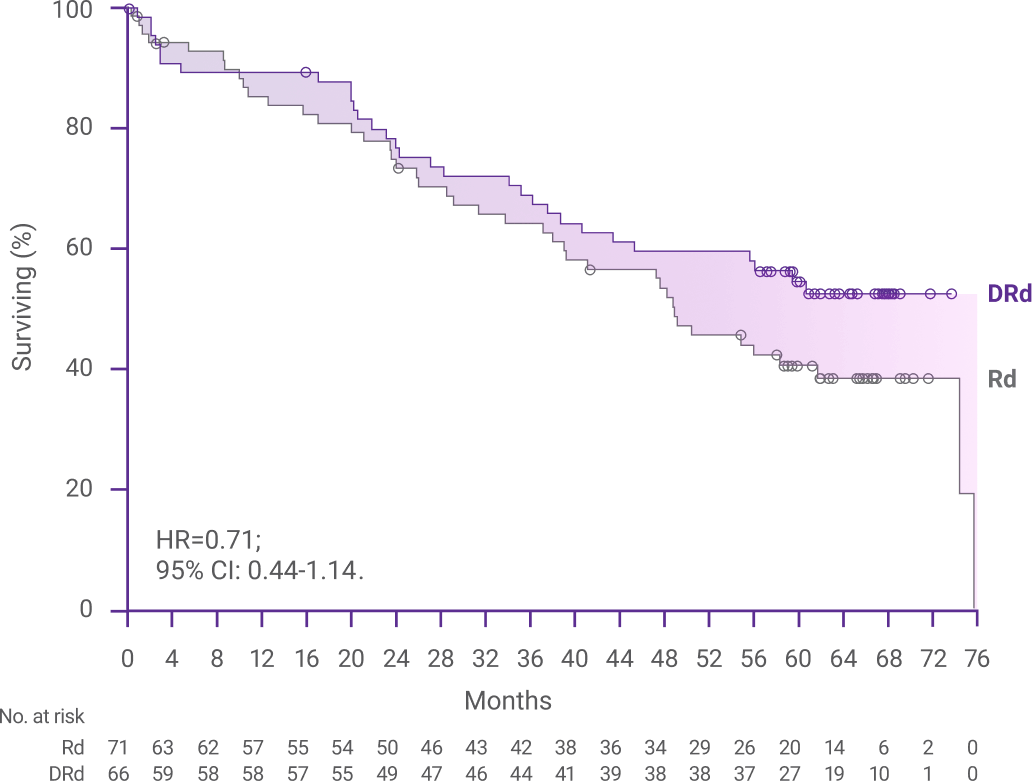
- Facon T, Moreau P, Weisel K, et al. Daratumumab/lenalidomide/dexamethasone in transplant-ineligible newly diagnosed myeloma: MAIA long-term outcomes. Leukemia. 2025;39:942-950.
- Facon T, Moreau P, Weisel K, et al. Daratumumab/lenalidomide/dexamethasone in transplant-ineligible newly diagnosed myeloma: MAIA long-term outcomes. Leukemia. 2025;39(4):942-950 [supplementary appendix].
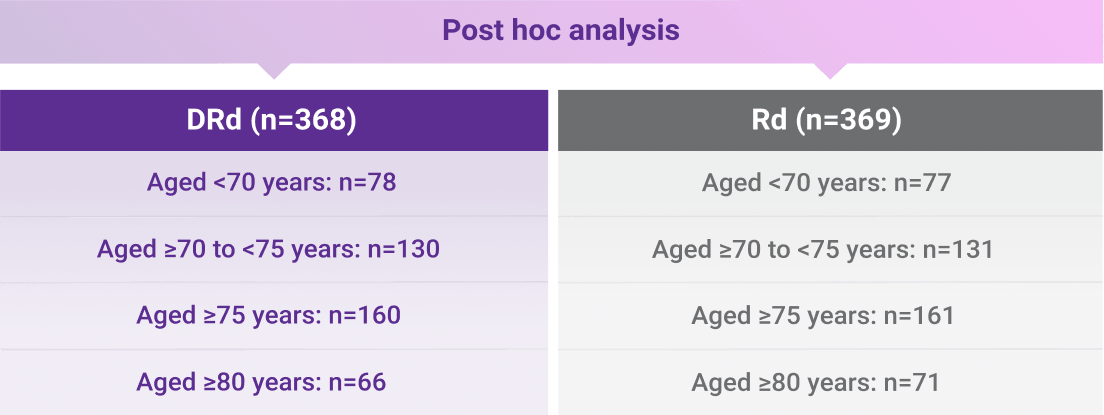
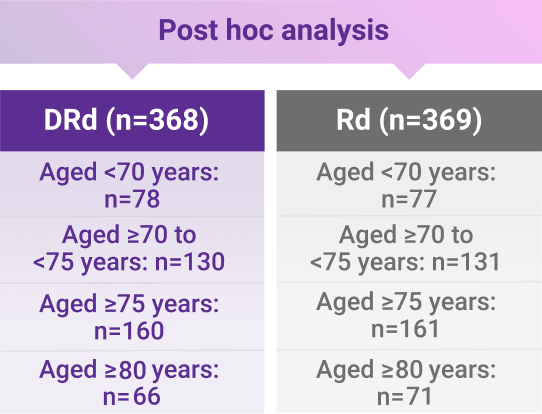
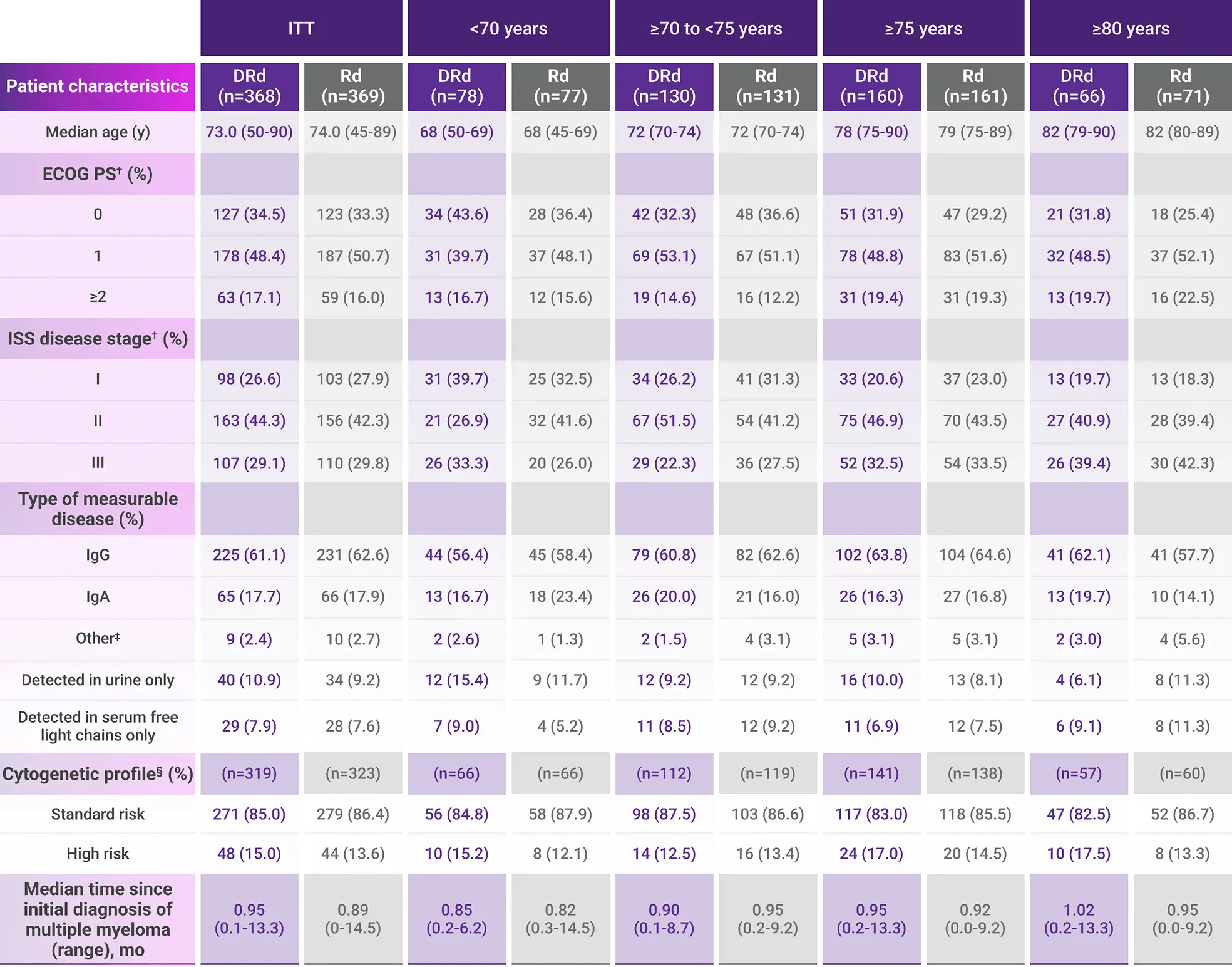
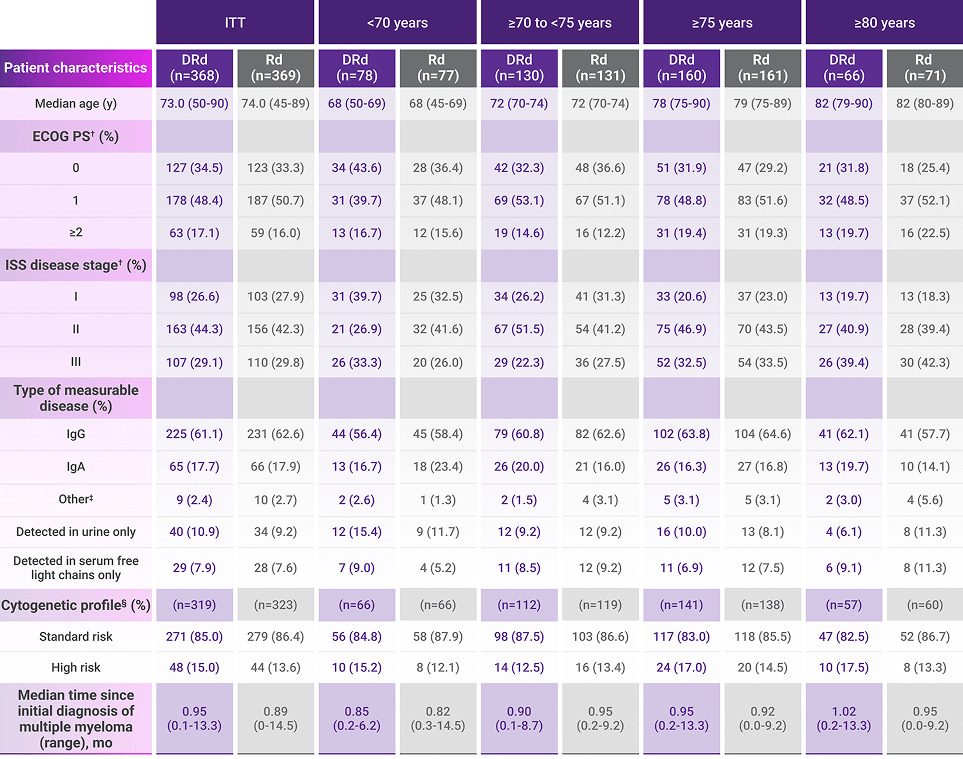
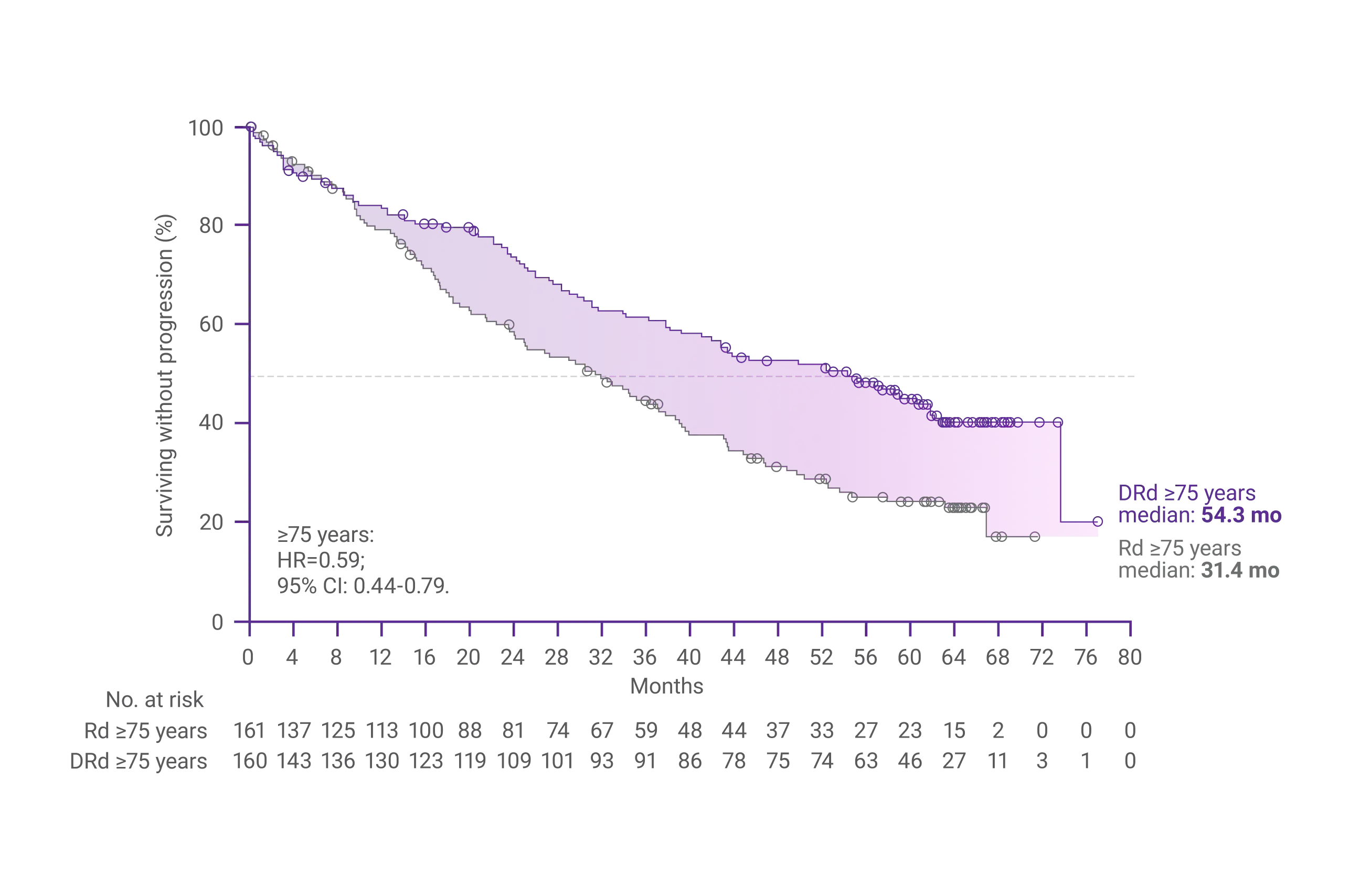
- Facon T, Kumar SK, Weisel K, et al. Daratumumab plus lenalidomide and dexamethasone in patients with transplant-ineligible newly diagnosed multiple myeloma: MAIA age subgroup analysis. Poster presented at: 64th American Society of Hematology (ASH) Annual Meeting & Exposition; December 10-13, 2022; New Orleans, LA.
- DARZALEX FASPRO® [Prescribing Information]. Horsham, PA: Janssen Biotech, Inc.
- Moreau P, Facon T, Usmani SZ, et al. Daratumumab plus lenalidomide and dexamethasone (D-Rd) versus lenalidomide and dexamethasone (Rd) in transplant-ineligible patients with newly diagnosed multiple myeloma (NDMM): clinical assessment of key subgroups of the phase 3 MAIA study. Poster presented at: 64th American Society of Hematology (ASH) Annual Meeting & Exposition; December 10-13, 2022; New Orleans, LA.