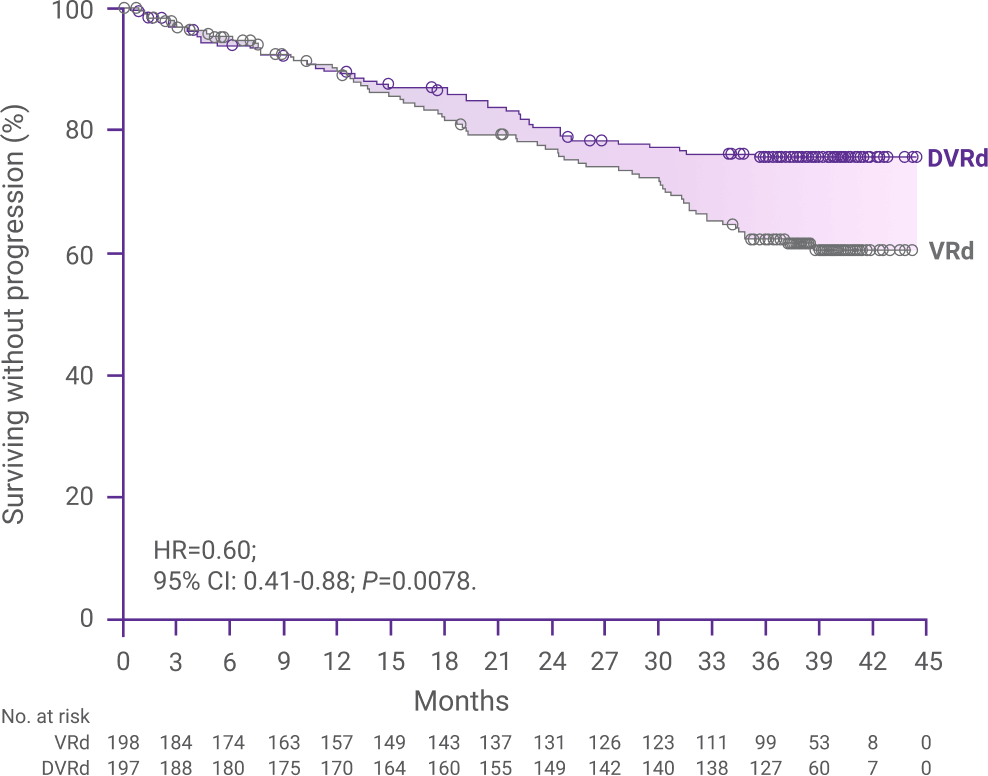
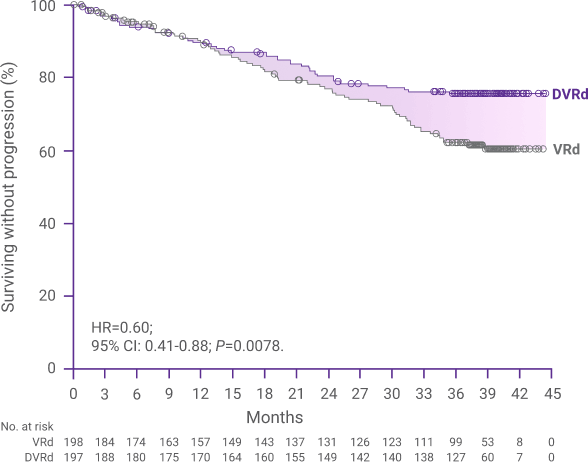
Primary Analysis (22 Months)
For transplant-ineligible patients with newly diagnosed multiple myeloma
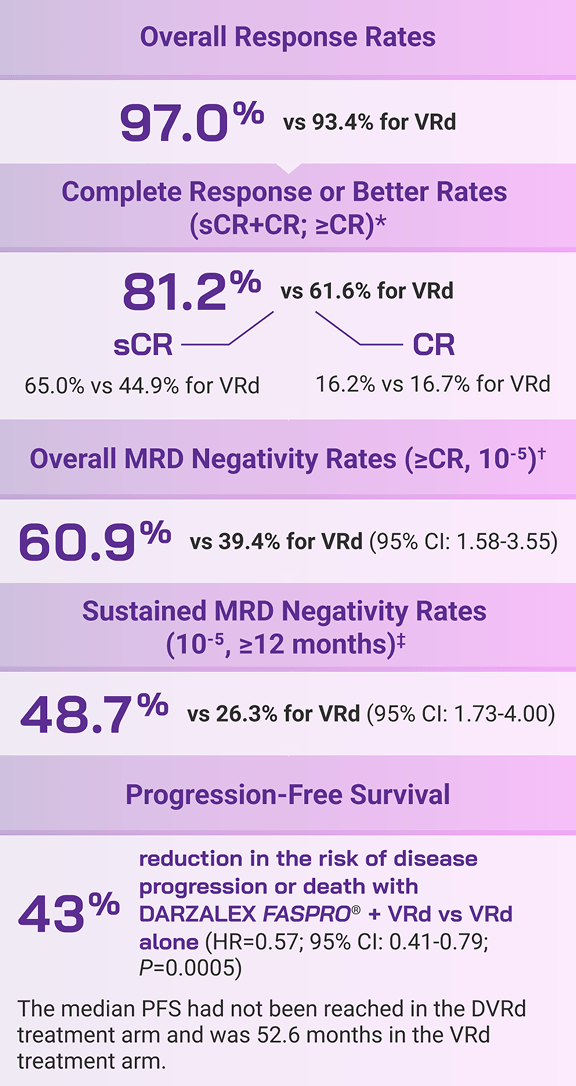
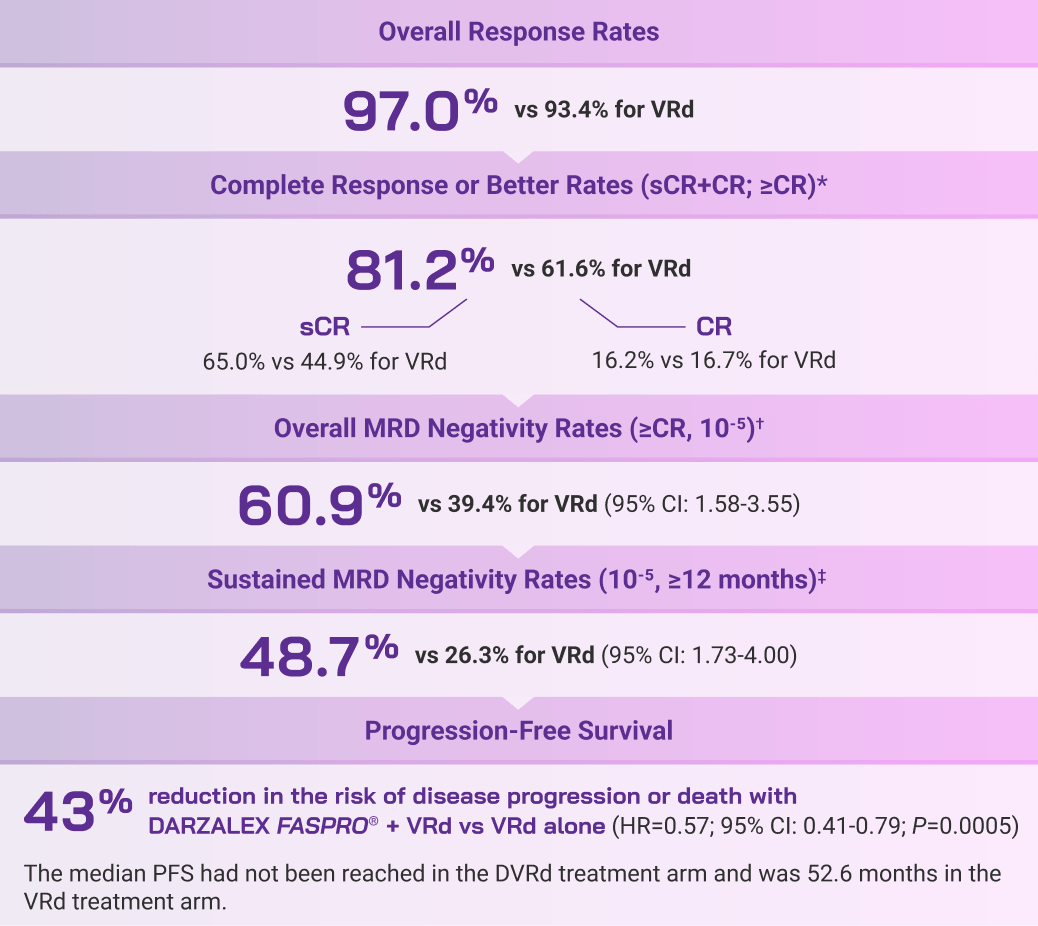
Deep responses
More patients achieved MRD negativity (10-5) and CR or better with DARZALEX FASPRO® + VRd vs VRd alone4*†
52%of patients achieved MRD negativity (10-5) and complete response or better with DVRd
vs(P=0.0005)
35%with VRd alone†‡
At a median follow-up of 22 months, overall complete response or better (≥CR) rates were 76.1% in the DVRd arm and 58.6% in the VRd arm (P=0.0002).§
CR=complete response; DVRd=DARZALEX FASPRO® (D) + bortezomib (V) + lenalidomide (R) + dexamethasone (d); MRD=minimal residual disease; VRd=bortezomib (V) + lenalidomide (R) + dexamethasone (d).
*At a median follow-up of 22 months.4
†Primary endpoint.4,5
‡MRD-negative complete response rate was defined as the proportion of patients who achieved both MRD negativity (10-5 threshold) and ≥CR.4
§Secondary endpoint.5