CEPHEUS Study Design


The CEPHEUS Study: DARZALEX FASPRO® + VRd
The first and only FDA approval in NDMM based on a study with a primary endpoint of MRD negativity (≥CR, 10-5)1-3
CEPHEUS: Phase 3 study of DARZALEX FASPRO® + VRd vs VRd in patients with newly diagnosed multiple myeloma who are ineligible for autologous stem cell transplant (ASCT) or refused transplant as initial therapy.1,3
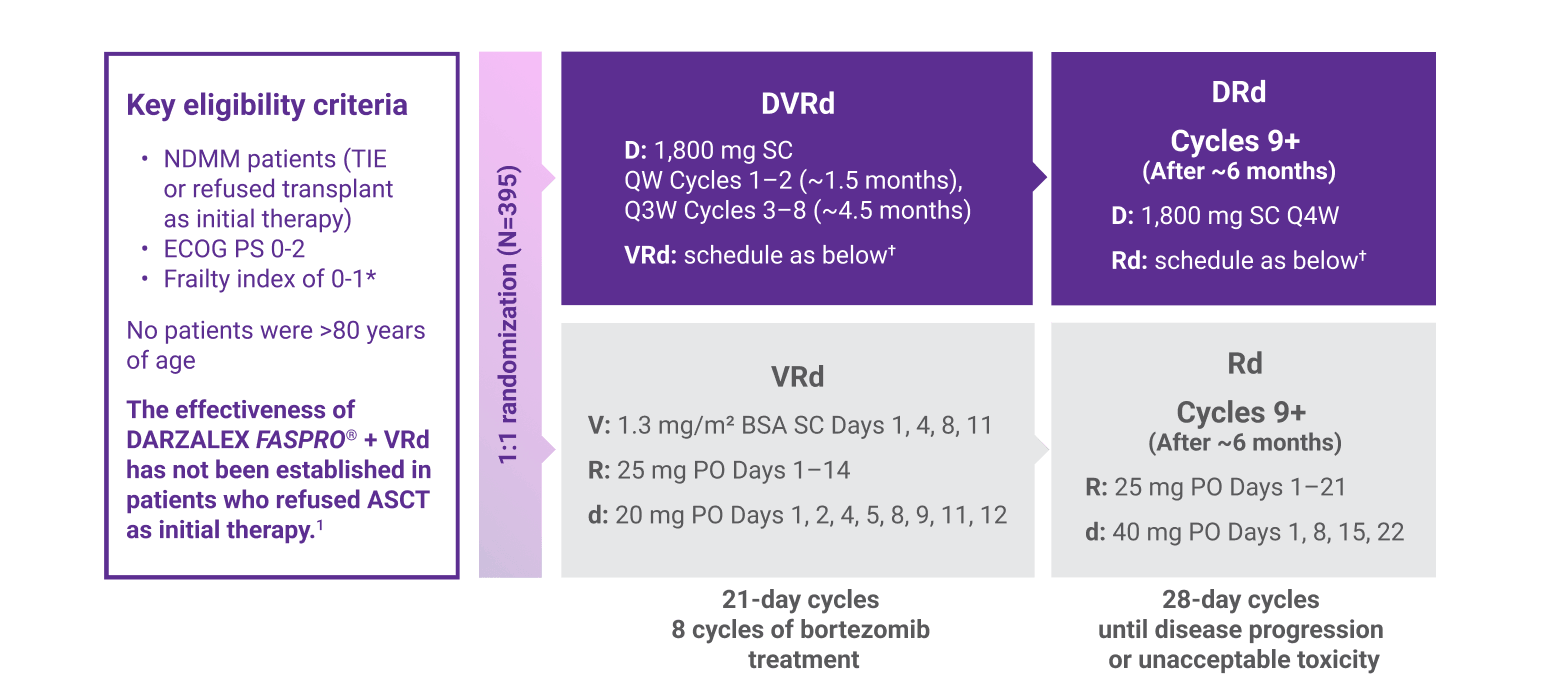
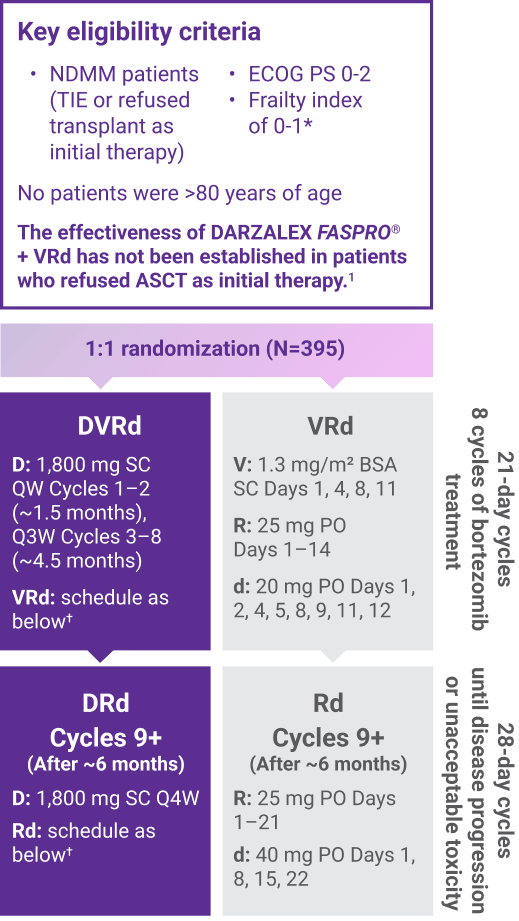
Primary endpoint:
Overall MRD (≥CR) negativity rate1,3‡
Key secondary endpoints included:
Complete response (CR) or better (≥CR) rate, progression-free survival, sustained MRD negativity (≥CR; 10-5) rate (≥12 months)1,3
ASCT=autologous stem cell transplant; BSA=body surface area; CR=complete response; D=DARZALEX FASPRO®; d=dexamethasone; DRd=DARZALEX FASPRO® (D) + lenalidomide (R) + dexamethasone (d); DVRd=DARZALEX FASPRO® (D) + bortezomib (V) + lenalidomide (R) + dexamethasone (d); ECOG PS=Eastern Cooperative Oncology Group performance status; FDA=U.S. Food and Drug Administration; MRD=minimal residual disease; NDMM=newly diagnosed multiple myeloma; PO=oral; QW=every week; Q3W=every 3 weeks; Q4W=every 4 weeks; R=lenalidomide; Rd=lenalidomide (R) + dexamethasone (d); SC=subcutaneous; TIE=transplant ineligible; V=bortezomib; VRd=bortezomib (V) + lenalidomide (R) + dexamethasone (d).
*Calculation of additive frailty is based on a scale of 0-5 based on age, comorbidities, and cognitive and physical conditions, with 0 indicating fit, 1 indicating intermediate fitness, and ≥2 indicating frail, per the Myeloma Geriatric Assessment score (http://www.myelomafrailtyscorecalculator.net).3
†On the days of DARZALEX FASPRO® injection, the dexamethasone dose was administered orally or intravenously as a pre-injection medication.1
‡FDA dictates that MRD should be assessed in patients who are in CR.4
CEPHEUS Patient Demographics
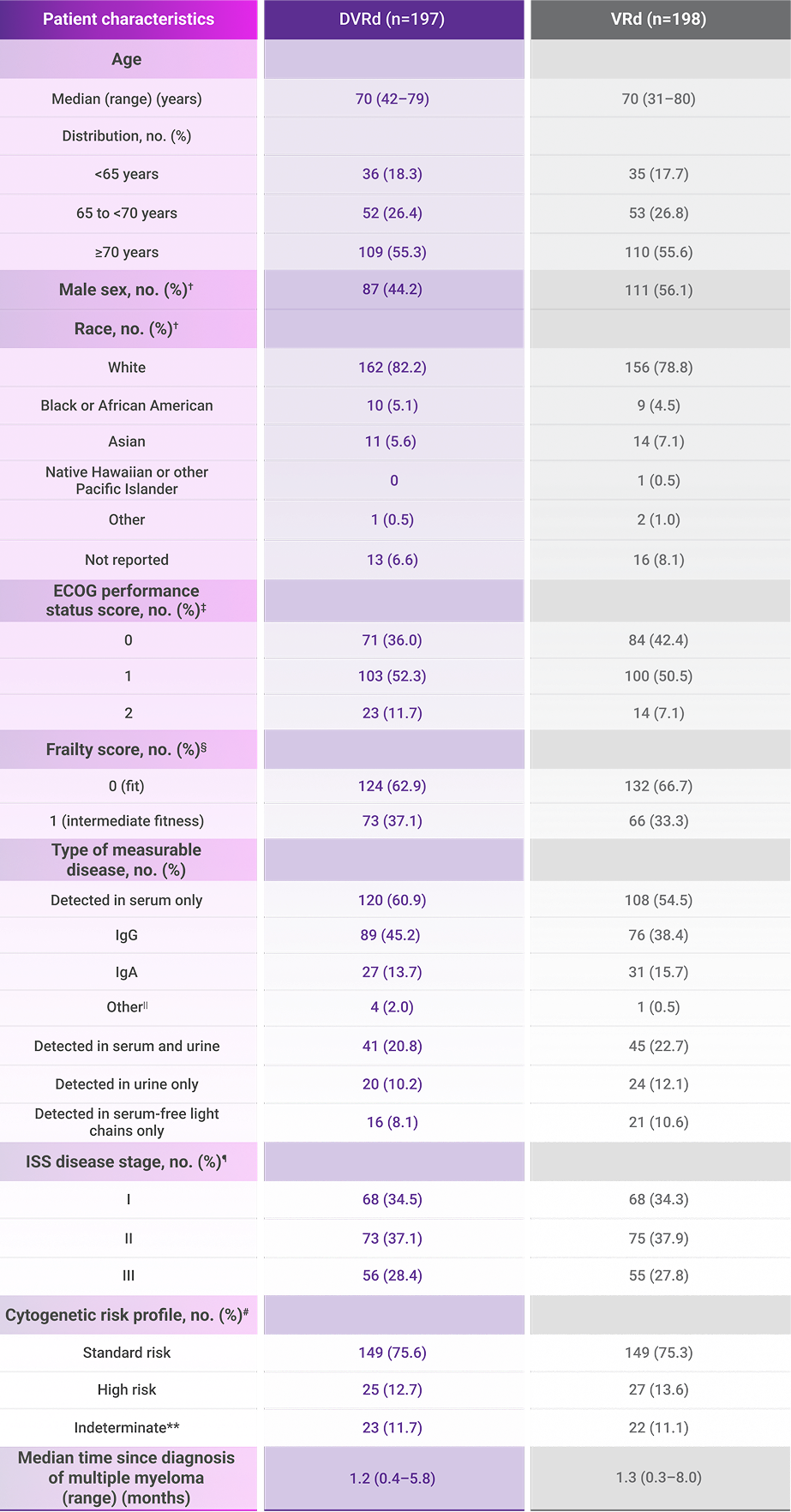
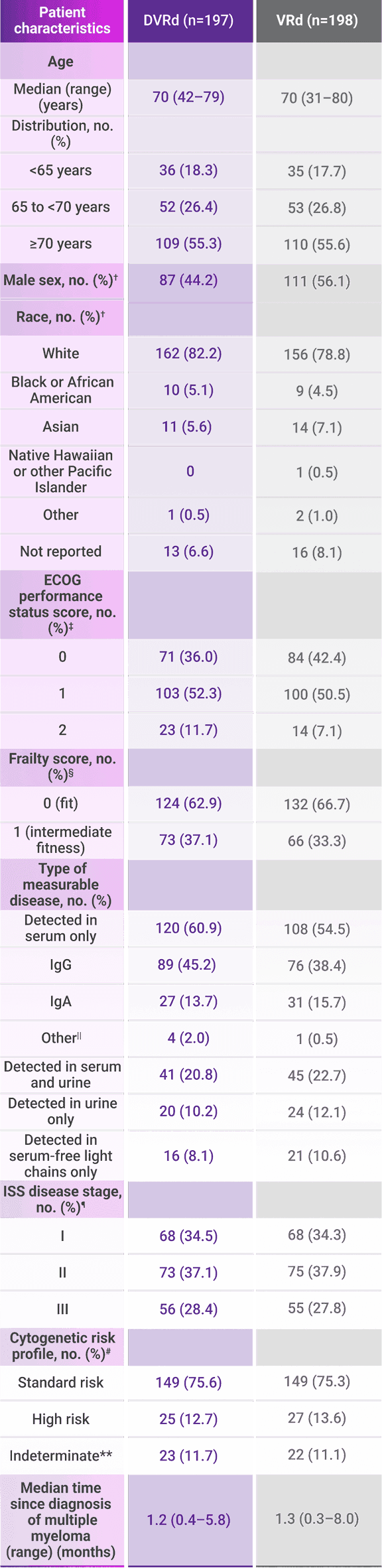
CEPHEUS: Patient demographics and clinical characteristics at baseline (ITT population)3*
CEPHEUS included a broad range of patients with newly diagnosed multiple myeloma1,3
DVRd and VRd treatment arms were well balanced3,5
In CEPHEUS, 21% of patients enrolled in the trial were aged 75 years and older1
del=deletion; DVRd=DARZALEX FASPRO® (D) + bortezomib (V) + lenalidomide (R) + dexamethasone (d); ECOG=Eastern Cooperative Oncology Group; IgA=immunoglobulin A; IgD=immunoglobulin D; IgE=immunoglobulin E; IgG=immunoglobulin G; IgM=immunoglobulin M; ISS=International Staging System; ITT=intent-to-treat; t=translocation; VRd=bortezomib (V) + lenalidomide (R) + dexamethasone (d).
*The intention-to-treat population was defined as all patients who underwent randomization.3
†Sex and race were reported by the patient.3
‡ECOG performance status is scored on a scale of 0-5, with 0 indicating no symptoms and higher scores indicating increasing disability.3
§Total additive frailty is scored on a scale of 0-5 based on age, comorbidities, and cognitive and physical conditions, with 0 indicating fit, 1 intermediate fitness, and ≥2 frail, per the Myeloma Geriatric Assessment score (http://www.myelomafrailtyscorecalculator.net).3
||Includes IgD, IgM, IgE, and biclonal.3
¶ISS disease stage is based on the combination of serum β2-microglobulin and albumin levels. Higher stages indicate more advanced disease.3
#Cytogenetic risk was assessed by fluorescence in situ hybridization. High risk was defined as the presence of del(17p), t(4;14), and/or t(14;16).3
**Indeterminate includes patients with missing or unevaluable samples.3


del=deletion; DVRd=DARZALEX FASPRO® (D) + bortezomib (V) + lenalidomide (R) + dexamethasone (d); ECOG=Eastern Cooperative Oncology Group; IgA=immunoglobulin A; IgD=immunoglobulin D; IgE=immunoglobulin E; IgG=immunoglobulin G; IgM=immunoglobulin M; ISS=International Staging System; ITT=intent-to-treat; t=translocation; VRd=bortezomib (V) + lenalidomide (R) + dexamethasone (d).
*The intention-to-treat population was defined as all patients who underwent randomization.3
†Sex and race were reported by the patient.3
‡ECOG performance status is scored on a scale of 0-5, with 0 indicating no symptoms and higher scores indicating increasing disability.3
§Total additive frailty is scored on a scale of 0-5 based on age, comorbidities, and cognitive and physical conditions, with 0 indicating fit, 1 intermediate fitness, and ≥2 frail, per the Myeloma Geriatric Assessment score (http://www.myelomafrailtyscorecalculator.net).3
||Includes IgD, IgM, IgE, and biclonal.3
¶ISS disease stage is based on the combination of serum β2-microglobulin and albumin levels. Higher stages indicate more advanced disease.3
#Cytogenetic risk was assessed by fluorescence in situ hybridization. High risk was defined as the presence of del(17p), t(4;14), and/or t(14;16).3
**Indeterminate includes patients with missing or unevaluable samples.3

Transplant-Ineligible Multiple Myeloma
NCCN Category 1, preferred*†
The NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) may contain data, conclusions, and recommendations that do not conform to the FDA-approved labeling for the products discussed herein and have not been evaluated by the FDA. No conclusions should be drawn. Daratumumab (DARZALEX®) and daratumumab and hyaluronidase-fihj (DARZALEX FASPRO®) should be used only as specified in the Prescribing Information.
Daratumumab‡ (D) in combination with bortezomib (V), lenalidomide (R), and dexamethasone (d) is recommended by the NCCN Guidelines® as a Category 1 preferred therapeutic option for patients with newly diagnosed multiple myeloma who are ineligible for transplant§ (for patients <80 years old who are not frail).6
The effectiveness of daratumumab and hyaluronidase-fihj (DARZALEX FASPRO®) + VRd has not been established in patients who refused autologous stem cell transplant as initial therapy.
FDA-Approved Indication
DARZALEX FASPRO® (daratumumab and hyaluronidase-fihj) + VRd is indicated for the treatment of newly diagnosed adult patients with multiple myeloma who are ineligible for autologous stem cell transplant.1
FDA=U.S. Food and Drug Administration; NCCN=National Comprehensive Cancer Network; VRd=bortezomib (V) + lenalidomide (R) + dexamethasone (d).
*See NCCN.org for definitions of NCCN Categories of Preference and NCCN Categories of Evidence and Consensus.
†Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Multiple Myeloma V5.2026. © National Comprehensive Cancer Network, Inc. 2026. All rights reserved. Accessed June 8, 2026. To view the most recent and complete version of the guideline, go online to NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or applications and disclaims any responsibility for their application or use in any way.
‡Daratumumab includes both daratumumab (DARZALEX®) for intravenous infusion and daratumumab and hyaluronidase-fihj (DARZALEX FASPRO®) for subcutaneous injection. Daratumumab and hyaluronidase-fihj for subcutaneous injection has different dosing and administration instructions compared with daratumumab for intravenous infusion.
§If hematopoietic cell transplantation (HCT)-deferred or not indicated.


References:
DARZALEX FASPRO® [Prescribing Information]. Horsham, PA: Janssen Biotech, Inc.
Data on file. RF-433969. Janssen Biotech, Inc.
Usmani SZ, Facon T, Hungria V, et al. Daratumumab plus bortezomib, lenalidomide and dexamethasone for transplant-ineligible or transplant-deferred newly diagnosed multiple myeloma: the randomized phase 3 CEPHEUS trial. Nat Med. 2025;31(4):1195-1202.
- Data on file. RF-140179. Janssen Biotech, Inc.
Usmani SZ, Facon T, Hungria V, et al. Daratumumab SC + bortezomib/lenalidomide/dexamethasone in patients with transplant-ineligible or transplant-deferred newly diagnosed multiple myeloma: results of the phase 3 CEPHEUS study. Presented at: 21st International Myeloma Society (IMS) Annual Meeting; September 25-28, 2024; Rio de Janeiro, Brazil.
Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Multiple Myeloma V.5.2026. © National Comprehensive Cancer Network, Inc. 2026. All rights reserved. Accessed March 25, 2026. To view the most recent and complete version of the guideline, go online to NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way.